
My Dentist Said I Need a Filling. Do I Actually Need One?

You go in for a check-up. No pain. Nothing visible. Then your dentist takes a set of bitewing radiographs, points to a shadow on the screen, and tells you that you need a filling.
It is a reasonable question to ask: do I actually need this?
The short answer is — it depends entirely on how deep that shadow goes. And most patients are never told the difference.
The RA Classification
Not all radiographic shadows are the same. In Australia, we commonly use the RA classification system to grade the depth of decay visible on a bitewing radiograph.
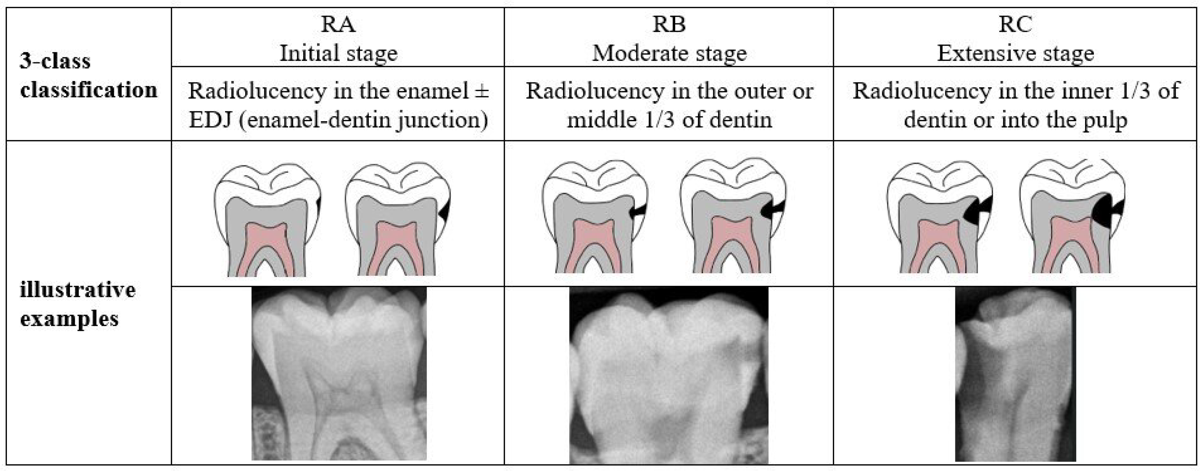
The RA classification system — grading decay depth from outer enamel (RA1) to pulp involvement (RA6)
| Grade | What it means | Recommended approach |
|---|---|---|
| RA1 | Radiolucency in the outer half of enamel | Monitor — no filling needed |
| RA2 | Radiolucency in the inner half of enamel | Monitor — remineralise first |
| RA3 | Radiolucency reaching the enamel-dentine junction (EDJ) | Clinical judgement — discuss options |
| RA4 | Radiolucency in the outer half of dentine | Filling recommended |
| RA5 | Radiolucency in the inner half of dentine | Filling required — do not delay |
| RA6 | Radiolucency into the pulp | Urgent treatment required |
The critical clinical question is: at what point does a shadow on a radiograph become a tooth that needs a filling?
What the Evidence Says
A Cochrane review (Ricketts et al., 2013) examined the management of early caries lesions and found that lesions confined to enamel (RA1–RA2) can often be managed non-operatively — with remineralisation strategies, dietary advice, and monitoring — without progressing to the point of needing a filling.
Schwendicke et al. (2016), in a consensus paper published in Advances in Dental Research, recommended non-operative management of caries confined to the enamel and even lesions reaching the outer third of dentine in low-risk patients. Their international expert panel concluded that operative intervention is most clearly justified when caries has progressed well into dentine — not at the first sign of a radiographic shadow.
More recently, Molyneux and Banerjee (2024) published a paper in the British Dental Journal on staging and grading carious lesions within a minimum intervention oral care framework. Their key argument: accurate assessment of lesion depth (staging) and whether the lesion is active or arrested (grading) should drive treatment decisions. They are explicit that intervening operatively at the wrong stage starts patients on an irreversible restorative cycle unnecessarily.
A systematic review of practitioner thresholds (Innes et al., updated 2025) found that globally, only 13% of dentists would restoratively manage a lesion confined to enamel. In Australia, that figure dropped to just 4%. However, for proximal lesions, intervention rates have actually increased since 2016 — suggesting that despite the evidence for conservative management, clinical behaviour is moving in the opposite direction for interproximal caries. This is a concerning trend.
These findings collectively suggest that for a significant number of early radiographic lesions, the filling may not be necessary — at least not yet.
Things to Consider
There are legitimate reasons a dentist may recommend a filling at RA3 or even RA2. Radiographs underestimate the true depth of a lesion. By the time a shadow reaches the EDJ on a bitewing, histological studies suggest the actual caries front may already be into dentine. Patient compliance with preventive regimens varies. And a clinician who has seen a patient’s lesion progress over two recall intervals may reasonably decide that monitoring has run its course.
There is also the practical reality that early intervention — when the lesion is small — means a smaller, more conservative filling. Waiting too long can mean a larger restoration, greater tooth structure loss, and higher long-term cost.
So this is not a case of fillings being unnecessary. Fillings are essential when caries has progressed into dentine. The question is whether every early radiographic shadow warrants operative treatment, or whether some can be safely monitored and reversed.
My Concerns
My concern is that in practice, the threshold for intervention is often too low. I have seen RA1 and RA2 lesions treated operatively when the evidence supports monitoring. Once a filling is placed, the tooth enters a restorative cycle — fillings fail, they get replaced with larger fillings, which fail, and eventually you are looking at a crown or worse. Every filling is the beginning of that cycle, and every unnecessary filling accelerates it.
There is also a financial incentive to treat. A monitored lesion generates a check-up fee. A filled lesion generates a restorative fee. I am not suggesting most clinicians are motivated by this, but the incentive structure exists and it is worth acknowledging.
My Advice
If your dentist tells you that you need a filling and you have no symptoms and cannot see anything wrong, ask one question: where is the decay on the radiograph, and what RA classification is it?
What to ask at your next appointment
Ask whether monitoring with fluoride varnish, tooth mousse (CPP-ACP) and improved oral hygiene is a reasonable alternative. In most cases, it is.
This is a clinical judgement call. Discuss the options, your risk profile, and whether the lesion has been stable or progressing over previous recalls.
Get the filling. The evidence clearly supports intervention at this stage, and delay risks a worse outcome including root canal treatment or tooth loss.
Do not refuse treatment out of fear. But do not accept it without understanding what you are being treated for.
Video coming soon — subscribe to our YouTube channel for updates.
References
- Ricketts D, Lamont T, Innes NP, et al. Operative caries management in adults and children. Cochrane Database of Systematic Reviews. 2013.
- Schwendicke F, Frencken JE, Bjørndal L, et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Advances in Dental Research. 2016;28(2):58–67.
- Molyneux E, Banerjee A. Staging and grading carious lesions within a minimum intervention oral care framework. British Dental Journal. 2024.
- Innes NP, et al. Practitioner thresholds for operative caries management: a systematic review update. PMC. 2025.
Dr Max has been practising dentistry for nearly 20 years. He is the principal dentist at Dental on Flinders and the director of dental technology company CoTreat and non-profit Medicare for Dental, where he works on dental policy and improving access to care in Australia.
Questions about your own dental health?
Book a check-up at Dental on Flinders — evidence-based, high-tech dentistry in the Melbourne CBD. Open 7 days, opposite Flinders Street Station.
Book an appointment